

Written by: Andrew Akhaphong, MS, RD, LD, Mackenthun’s Registered Dietitian
Updated: January 9, 2024
Intro to Magnesium
Magnesium is one of the most abundant mineral in the human body; approximately 40% are stored in intracellular space while 60% are stored in the bones and teeth.1 Evidence suggests that 1% of magnesium however is found in the blood.2 Its purpose includes maintaining cellular function such as promoting DNA and RNA synthesis, regulating antioxidant binding capacity, acting as a cofactor for over 300 enzymes including for the metabolism of the amino acid glutathione, and support muscle contraction.3

Sources of Magnesium
The highest sources of magnesium include dark green cruciferous vegetables, fortified cereal, whole grains, nuts, seeds, bananas, and legumes. Additionally, drinking water in the United States is also a source of magnesium.
The recommended daily allowance for magnesium is 4.5 milligrams per kilogram body weight a day for adults.4 Additionally the upper tolerable upper limit is no more than 420 milligrams per day for adult males and 350 milligrams per day for adult females (including pregnant and lactating).5
Absorption and Reabsorption of Magnesium
The primary sites of magnesium absorption are the jejunum, ileum, and the colon. Here, about 30-40% of magnesium are absorbed; however, intestinal absorption can be inversely related to intake influenced by homeostasis.4 Current evidence states that at low intake of magnesium, it is approximately 65% while high intake of magnesium it is about 11%.6 Current research is limited in the understanding of magnesium absorption though. It is theorized that parathyroid hormone may regulate magnesium absorption or be influenced by Vitamin D3.7
In relation to homeostasis the kidney is the largest influencer in maintaining serum levels of magnesium through urinary excretion and reabsorption. Reabsorption of magnesium occurs through the proximal tubule (20%), the cortical thick ascending limb (60%), and the distal convoluted tubule (5-10%).8,9
Evidence suggests there are nutrient-nutrient interactions that influence magnesium absorption. One example is when calcium intake is low and magnesium is high, this allows for the activation of magnesium transporters through the intestine; however, the inverse can occur reducing the rate of magnesium absorption.10 Zinc in the other hand, may improve magnesium absorption. In a small sample size of 55 participants with coronary heart disease and type-2 diabetes, 27 participants were given 250 milligrams of magnesium oxide and 150 milligrams of zinc sulfate while the remainder took a placebo for 12-weeks. The following results occured –11
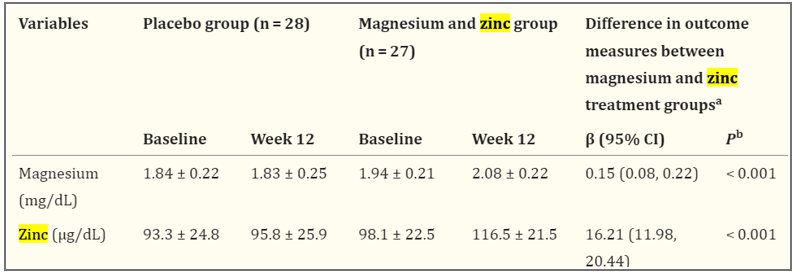
While the data shows this is significant, it is important to note that the sample size is small and this was a result in persons with chronic heart disease and type-2 diabetes.
Integrative Intervention of Magnesium: Sleep
Studies suggest that magnesium may support sleep through the expression of the glutamatergic and gamma-aminobutyric acid (GABA) ergic system.12 Additionally magnesium may suppress N-methyl-D-asoartate receptors to promote muscle relaxation to improve sleep.7 Though limited human studies exist, rat models suggest magnesium deficiency resulted in decreased serum melatonin levels.13
In a study of 3,964 participants with depressive disorders or an absent of depressive disorders were recruited through the Coronary Artery Risk Development in Young Adults project.12 The researchers had the participants self-report their sleep quality through a Likert scale from one to five (very good to very poor). The participants also completed a food frequency questionnaire to assess for magnesium and calcium intake (due to their synergistic effects). It is important to note that subjective data like this has room to skew data. These participants were followed for four quarters and no participants dropped out during the duration of the study. Additionally serum magnesium levels and serum calcium levels were measured each quarter and compared to their sleep quality.
Results from the study show that persons with higher intake of magnesium and calcium exhibited improved sleep of greater than seven hours per night; however, it was noted this significance was among groups with no depressive disorders.12 Serum calcium and magnesium levels showed no significant difference among persons with depressive disorders in sleep quality or sleep duration.12
In the elderly it is known that this population may be at higher risk for nutritional deficiencies due to loss of independence, appetite changes, metabolic or organ functioning changes, and side effects from medications. In a double-blind placebo-controlled trial published in 2012, 46 elderly persons were followed for eight weeks.14 The participants were also tested for serum cortisol levels before and after experimentation, as stress may influence sleep quality and sleep duration. The experimental group received 500 milligrams of magnesium oxalate while the control group received 500 milligrams of a placebo. Results report that the experimental group showed improved sleep quality and an average sleep duration of greater than seven hours per night while the placebo group reported poor sleep quality and an average sleep duration of five hours per night. Not surprisingly, the experimental group also exhibited reduced serum cortisol levels. It is important to note in this study that two participants did not take their magnesium supplementation as prescribed and the dropout rate was 6.5%.
Integrative Intervention of Magnesium: Insulin Resistance
Current studies report that persons with type-2 diabetes often have low serum magnesium levels. Therefore, some studies suggest magnesium supplementation can be beneficial in persons with type-2 diabetes while other studies disagree. It is important to note that limited studies exist around this topic at this time.
A study in 2020 reports that magnesium improves beta-cell functioning of the pancreas by promoting the NIPAL-1 enzyme. If one recalls, magnesium is important in gene expression.15 In additional study reports that magnesium deficiency decreases Vitamin D3’s ability to improve HOMA-beta functioning and increase risk for beta-cell dysfunction.16
Rodriguez-Moran and Guerrero-Romero investigated the effects of magnesium supplementation on insulin sensitivity and metabolism of persons with type-2 diabetes through a randomized double-blind controlled trial.17 Sixty-five participants with type-2 diabetes were organized into the control group where they received a placebo, or the experimental group which they received supplementation of magnesium chloride (50 grams per 1,000 mL solution); it is reported that magnesium chloride solution provides higher bioavailability than magnesium oxide. The study was done over the duration of 18-weeks. The lab values including fasting insulin, HgbA1c%, HOMA-IR index, and fasting blood glucose were measured. The following results occurred –
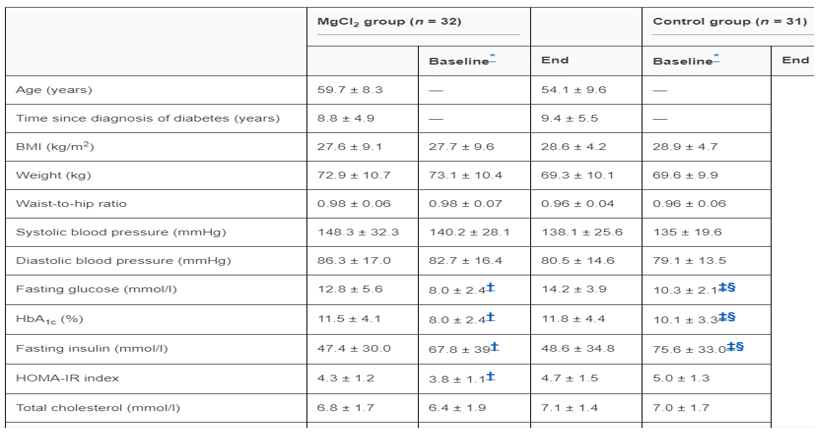
In the experimental group, significant improves were found in fasting insulin, HgbA1c, fasting blood glucose, and HOMA-IR index. It is important to note that there is an error in the design of the table above. The unidentified column under the experimental group is the “end” result while there is an extra empty “end” result column under the control group that is not needed.
Nutritional Considerations
There currently is no consensus at this time for dosing recommendations on magnesium to support sleep and/or insulin sensitivity; however, if dosing is not above the tolerable upper limit (420 milligrams/day for adult males and 350 milligrams/day for adult females), then it is assumed benefits will occur and magnesium toxicity risk will be reduced.
To ensure consumer safety, please look for supplements that contain the United States Pharmacopeia (USP) seal on the product. This is a third-party verification organization that follows Food and Drug Administration guidelines; in addition to, USP best practices for consumer safety. This includes validity of dose, validity of ingredients, risk of adulteration, and intended effects of the dose.

Scientific References:
- Houllier, P. Mechanisms and
regulation of renal magnesium transport. Annual Review of Physiology.
2014. 76:411-430. doi.org/10.1146/annurev-physiol-021113-170336
- Elin, R. J. Magnesium
metabolism in health and disease. Disease-a-Month. 1988. 34(4):166-218.
doi.org/10.1016/0011-5029(88)90013-2
- Razzaque, M. S. Magnesium: Are
we consuming enough?. Nutrients. 2018. 10(12). doi.org/10.3390/nu10121863
- Won Seo, J., Jin Park, T.
Magnesium metabolism. Electrolyte Blood Press. 2008. 6(2):86-95. doi:
10.5049/EBP.2008.6.2.86
- Office of Dietary Supplements.
Magnesium. Updated June 2, 2022. Accessed January 9, 2024.
https://ods.od.nih.gov/factsheets/Magnesium-HealthProfessional/
- Kayne, L. H., Lee, D. B.
Intestinal magnesium absorption. Mineral and Electrolyte Metabolism. 1993.
19(4-5):210-217. https://europepmc.org/article/med/8264506
- Swaminathan, R. Magnesium
metabolism and its disorders. Clin Biochem Rev. 2003. 24(2):47-66. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1855626/
- Quamme, G. A., Rabkin, S. W.
Cytosolic free magnesium in cardiac myocytes: identification of a Mg2+
influx pathway. Biochem Biophys Res Commun. 1990. 167(3):1406-12. doi:
10.1016/0006-291x(90)90679-h.
- Yu, A. S. Evolving concepts in
epithelial magnesium transport. Curr Opin Nephrol Hypertens. 2001.
10(5):649-53. doi: 10.1097/00041552-200109000-00016
- Hardwick, L. L., Jones, M. R.,
Brautbar, N., Lee, D. B. Magnesium absorption: mechanisms and the
influence of Vitamin D, calcium, and phosphate. 1991. 121(1):13-23. doi:
10.1093/jn/121.1.13
- Hamedilfard, Z., Farrokhian,
A., Reiner, Z., Bahamani, F., Asemi, Z., Ghotbi, M., Taghizadeh, M. The
effects of combined magnesium and zinc supplementation on metabolic status
in patients with type 2 diabetes mellitus and coronary heart disease.
Lipids Health Dis. 2020. 19:112. doi: 10.1186/s12944-020-01298-4
- Zhang, Y., Chen, C., Lu, L.,
Knutson, K. L., Carnethon, M. R., Fly, A. D., Luo, J., Haas, D. M.,
Shikany, J. M., Kahe, K. Association of magnesium intake with sleep
duration and sleep quality: findings from the CARDIA study. Sleep. 2021.
45(4). doi.org/10.1093/sleep/zsab276
- Billyard, A. J., Eggett, D. L.,
Franz, K. B. Dietary magnesium deficiency decrease plasma melatonin in
rats. 2006. Magnes Res. 19(3):157-61. https://pubmed.ncbi.nlm.nih.gov/17172005/
- Abbasi, B., Kimiagar, M.,
Sadeghniiat, K., Shirazi, M. M., Hedayati, M., Rashidkhani, B. The effect
of magnesium supplementation on primary insomnia in elderly: A
double-blind placebo-controlled clinical trial. J Res Med Sci. 2012.
17(12):1161-1169. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3703169/
- Manialaway, Y., Kham, S. R.,
Bhattacharjee, A., Wheeler, M. B. The magnesium transporter NIPAL1 is a
pancreatic islet-expressed protein that conditionally impacts insulin
secretion. 2020. J Biol Chem. 295(29):9879-9892. doi:
10.1074/jbc.RA120.013277
- Gong, R., Liu, Y, Luo, G.,
Yang, L. Dietary magnesium intake affects the Vitamin D effects on
HOMA-beta and risk of pancreatic beta-cell dysfunction: A cross-sectional
study. Front. Nutr. 2022. 9. doi.org/10.3389/fnut.2022.849747
- Rodriguez-Moran, M.,
Guerrero-Romero, F. Oral magnesium supplementation improves insulin
sensitivity and metabolic control in type 2 diabetic subjects: A
randomized double-blind controlled trial. Emerging Treatments and
Technologies. 2003. 26(4):1147-1152.
https://diabetesjournals.org/care/article/26/4/1147/23730/Oral-Magnesium-Supplementation-Improves-Insulin